
-
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
Publish Your Research/Review Articles in our High Quality Journal for just USD $99*+Taxes( *T&C Apply)
Offer Ends On
H. Bezza*, Z. Algouti, A. Mounsif, Y. Bennouk, L. Ait Lhaj, M. Kriet and F. Elasri
Corresponding Author: Houda B, Department of Ophthalmology, Avicenna military hospital of Marrakech, Morocco.
Received: November 02, 2023 ; Revised: November 05, 2023 ; Accepted: November 08, 2023 ; Available Online: November 17, 2023
Citation: Bezza H, Algouti Z, Mounsif A, Bennouk Y, Ait Lhaj L, et al. (2023) Isolated Ocular Rosacea in Children: Case Report. J Clin Ophthalmol Optom Res, 2(1): 1-3.
Copyrights: ©2023 Bezza H, Algouti Z, Mounsif A, Bennouk Y, Ait Lhaj L, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Views & Citations
Likes & Shares
We report the case of a 7-year-old child who presented to our department with recurrent red eye. After several investigations, the diagnostic of isolated ocular rosacea was retained and the patient was treated with local and general macrolide.
The evolution was marked by a complete remission of her symptoms and an improvement in her visual acuity.
Keywords: Ocular rosacea, Children, Optical coherence tomography, Morbidity
INTRODUCTION
Rosacea is a relatively common disease that can be confusing and lead to serious ocular morbidity if not correctly diagnosed and treated. Ocular rosacea, in particular, often goes undetected because there is no specific test to confirm it. Diagnosis is further complicated by the fact that ocular rosacea symptoms are not always typical of the disease. Further difficulties come from the fact that the severity of ocular symptoms often does not correlate with skin symptoms. It usually requires a combination of conservative measures and topical and systemic agents, depending on the severity of the disease.
CASE PRESENTATION
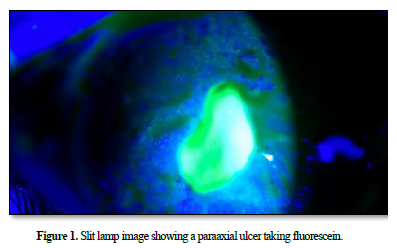
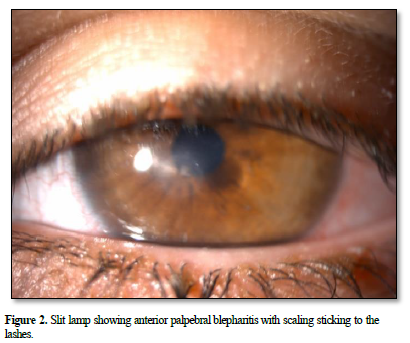
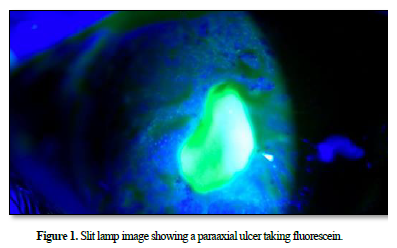
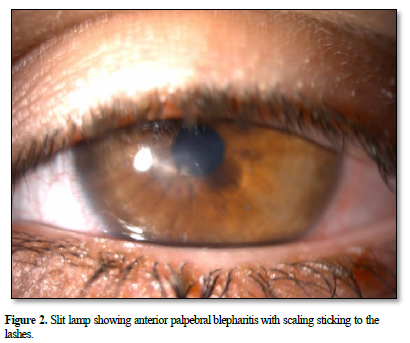
A 7-year-old girl who presented to our department with repeated left red eye over the 06 months. On the initial examination, best corrected visual acuity (BCVA) was 10/10 in the right eye and 03/10 in the left eye. Slit lamp bio microscopy revealed meibomitis, conjunctival hyperemia and a sterile para-axial corneal ulcer (Figures 1 & 2). The anterior chamber was quiet.
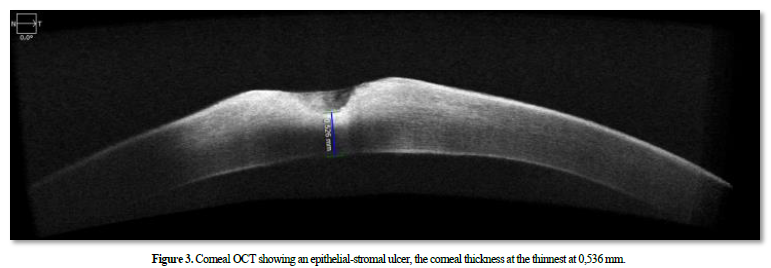
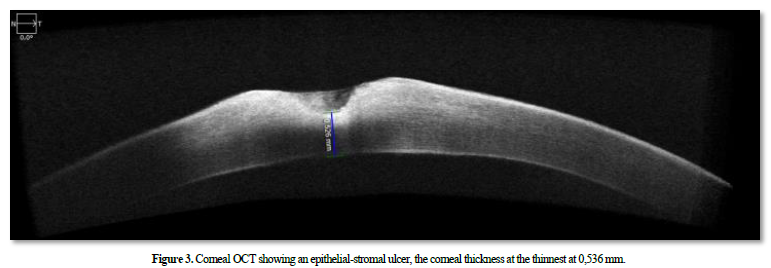
Fundus examination appeared normal. The examination of the right eye was unremarkable. The anterior segment optical coherence tomography (OCT) revealed an epithelial-stromal ulcer, the corneal thickness at the thinnest at 0,536 mm (Figures 3).
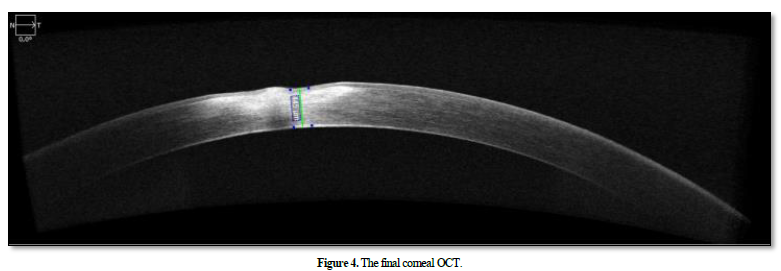
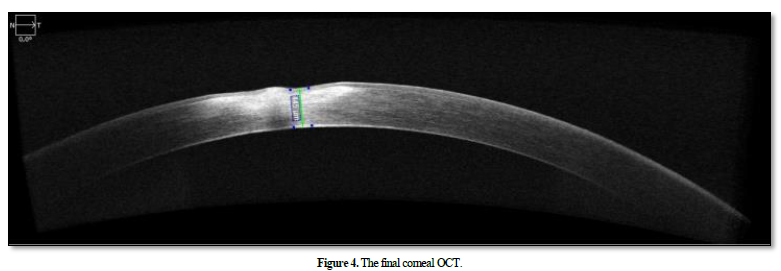
A sample was taken from the patient who came back negative, a complete biological check-up including immunological serological to search for systemic diseases was normal we treated the patient with antibiotic eye drops based on azithromycin for 6 months, Short-term local corticosteroid, palpebral hygiene measures with warm compresses and a general treatment based on macrolide for a period of 03 months. The patient was evaluated every single month for possible deterioration with a close follow-up with corneal OCT (Figure 4). Her BCVA improved from 3/10 to 08/10.
DISCUSSION
Rosacea is a chronic inflammatory dermatologic condition that is associated with ocular disease in approximately 58% of cases, although its precise pathophysiology remains unclear [1-3].
Studies have shown elevated levels of interleukin-1a and -b and increased gelatinase B (metalloproteinase [MMP]-9) and collagenase-2 (MMP-8) activity in tear fluids of patients with ocular rosacea. Doxycycline, which decreases MMP-8 and MMP-9 activity, has been used successfully in the treatment of cutaneous and ocular rosacea, confirming the inflammatory nature of the disease [4-6]. Ocular manifestations are usually bilateral, although unilateral or sequential changes may occur. Symptoms usually include ocular irritation, itching, redness, photophobia and/or epiphora, and reduced vision in the presence of corneal involvement [1,7]. Many groups have been investigating the glycomics of tear fluid and saliva in rosacea patients. This is a preliminary step in the search for a disease-specific biomarker, they reported a high abundance of O-linked oligosaccharides and a decrease in N-glycans in tear and saliva samples from rosacea patients [4,8]. Depending on the severity of the disease, treatment usually consists of a combination of conservative measures, topical agents and systemic agents. The use of oral cyclins is not recommended in children under 7 years of age. In these cases, oral erythromycin, 500 mg per day (as erythromycin) in divided doses for children may be used as an alternative. Alternatively, azithromycin 5 mg/kg/day orally for children, 3 days a week for 3 to 4 weeks [9,10].
CONCLUSION
In pediatric patients, ocular rosacea should be suspected in the presence of ocular surface disease associated with meibomitis.
Management of the disease can vary from local therapy to systemic treatment, according to the severity of the disorder. Visual impairment and resulting amblyopia are common and corneal perforation, although rare, is the most feared complication.

No Files Found




Internationally Accepted
Share Your Publication :